Visit profiles to view data profiles on chronic and disabling conditions and on young retirees and older workers.
A chronic condition that limits activities
Chronic Obstructive Pulmonary Disease, or COPD, includes chronic bronchitis and emphysema, two lung diseases that often coexist. In 1998, an estimated 9 million people were diagnosed with chronic bronchitis and another 3 million were living with emphysema. COPD is the fourth leading cause of death in the United States. The annual cost of COPD in the United States is estimated at $32.1 billion; health care expenditures account for $18 billion and indirect costs account for the other $14.1 billion.(1) People who have the condition are more likely to be limited in activities and less likely to be working than people who do not have COPD. They also have higher rates of health care service use. Smokers and people with asthma are particularly at risk of developing COPD.This Profile examines the characteristics of adults who report having chronic bronchitis, emphysema or COPD — referred to as “people with COPD.” Adults who do not report these diseases are referred to as “people without COPD.”
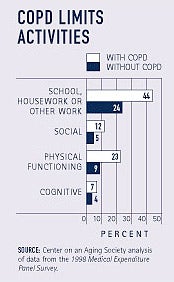
COPD limits activities for adults
Cognitive, physical, social and activity-related limitations are more prevalent among people who have COPD compared to those who do not have the con-dition. For example, almost twice as many people with COPD as without report that they are limited in school, housework or other work activities. A recent American Lung Association survey of hundreds of people living with the disease found that nearly half became short of breath while washing, dressing, or doing light housework. Over one-quarter — 28 percent — of respondents reported difficulty breathing even while sitting or lying still.(2)
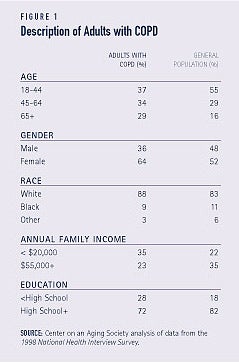
Who has COPD?
Among adults reporting COPD, the proportions of older people, women, whites, and people with low-incomes are higher than in the general population (see Figure 1). Of particular note is the larger proportion of women with COPD–women account for almost two-thirds of the population with the disease, but only about half of the general population. Since 1987 women have had higher rates of COPD than men, and in 2000, for the first time, the number of women who died from COPD was greater than the number of COPD deaths among men.(3)
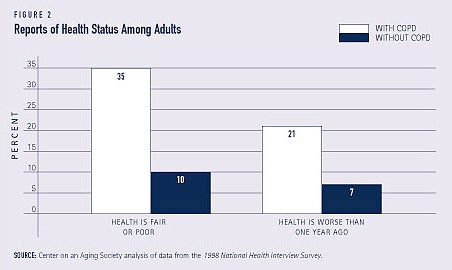
Poor health is associated with COPD
People with COPD are more than three times as likely as people who do not have the condition to say they are in fair or poor health. They are also three times more likely to report that their health status has deteriorated in the past year — 21 percent of people reporting COPD compared to 7 percent of people not reporting the condition (see Figure 2).
WHAT IS COPD?
COPD is an umbrella term for a group of diseases that includes chronic bronchitis and emphysema. COPD is characterized by obstruction to airflow and is not reversible. The primary symptoms of the disease are a chronic cough, shortness of breath, chest tightness, increased mucus production, and frequent clearing of the throat. The American Lung Association estimates that in addition to the people who have been diagnosed with the disease, there are 16 million undiagnosed individuals.
Chronic bronchitis and emphysema differ in the way in which they cause airflow obstruction of the lungs. Bronchitis is an inflammatory disease of the lining of the bronchial tubes, the tubes that connect the windpipe and the lungs. As they become inflamed, and often infected, less air is able to move to and from the lungs and heavy mucus is coughed up. Bronchitis starts in the small airways of the lungs and advances to the larger airways. Emphysema causes lung damage by inhibiting the ability of the lungs’ air sacs to stretch and recoil. The subsequent weakening and breaking of the air sacs causes air to be trapped and impairs the exchange of oxygen and carbon dioxide. Also, airflow is obstructed because the support of the airways is lost.4
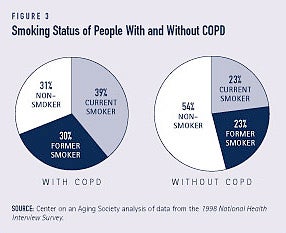
Tobacco is a key risk factor for COPD
Tobacco is a key risk factor in the development and progression of COPD — almost 70 percent of people who have COPD currently smoke or smoked at one time. In contrast, fewer than 50 percent of adults without COPD are current or former smokers (see Figure 3). The Centers for Disease Control and Prevention reports that the increasing trends in COPD rates and deaths among women reflects the increase in smoking by women, relative to men, in the United States.5
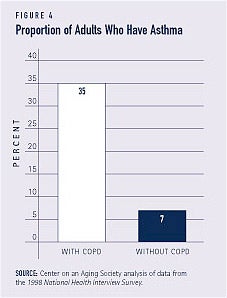
Asthma is related to COPD
A history of asthma is also associated with COPD. For example, more than one in three people who report COPD also have asthma while fewer than one in ten people without COPD have asthma (see Figure 4). People who have COPD and asthma are also more likely to have had a recent asthma episode or attack than people who have asthma but don’t have the disease. In addition to smoking and asthma, frequent respiratory infections and exposure to pollutants in the home and workplace also increase the risk of developing COPD.
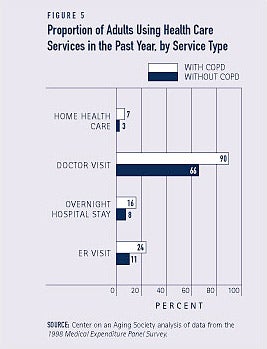
People who have COPD use more health care services
Health care service use is higher for people reporting COPD than for those without the condition. This is true for emergency room visits, overnight hospital stays, doctor visits and home health care visits (see Figure 5). For example, almost one in four adults with COPD had an ER visit during the past year while only about one in ten adults without the disease visited the ER. The proportion of people with COPD using home health care was more than twice as high as the proportion of people without the disease.
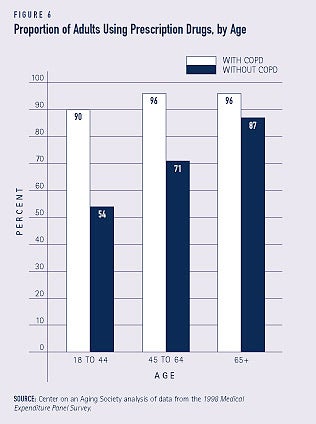
Prescription drug use is also higher
People who have COPD are much more likely to use prescription drugs than people who don’t have the disease–94 percent and 65 percent respectively. Prescription drug use is higher for those with COPD than for those without the condition regardless of age, though the differences narrow for older age groups (see Figure 6).
Some people with COPD may not get all the medication they need. For example, over one-tenth of adults age 51 and older who have COPD report that they delay taking medications or filling their prescriptions because of the cost.
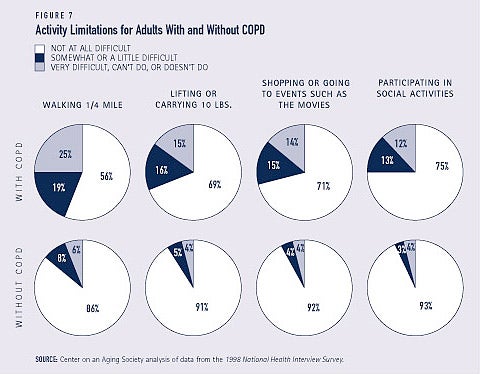
COPD affects daily life
COPD has a significant impact on people’s daily activities. Adults who have the condition are more likely than people who do not have COPD to say that, without special equipment, they have difficulty lifting or carrying 10 pounds, walking 1Ž4 mile, going shopping, or attending events (see Figure 7).
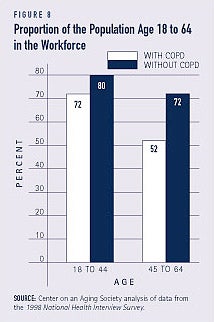
Employment rates are lower for people with COPD
Among adults under age 65, those who have COPD are less likely than those without the condition to be in the workforce — 62 percent compared to 77 percent. This is particularly true for those between ages 45 and 64 (see Figure 8).
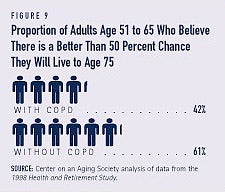
COPD affects adults’ outlook on longevity
Older adults who have COPD are far less optimistic about their longevity than people who do not have the condition. A larger proportion of adults age 51 to 65 without COPD than with COPD believe there is a greater than 50 percent chance they will live to age 75 (see Figure 9).
1.National Institutes of Health National Heart, Lung, and Blood Institute. (2002). Morbidity & Mortality: 2002 Chart Book on Cardiovascular, Lung, and Blood Diseases.
2. American Lung Association. (2001). Breathless in America: New Survey Reveals Impact of Chronic Obstructive Pulmonary Disease. Available at www.lungusa.org.
3. Centers for Disease Control and Prevention (2002). Chronic Obstructive Pulmonary Disease Surveillance–United States, 1971-2000. Morbidity and Mortality Weekly Report; 51.
4. American Lung Association. (2002). Diseases A to Z: Fact Sheets on Emphysema and Chronic Bronchitis. Available at www.lungusa.org.
5. Centers for Disease Control and Prevention (2002).
ABOUT THE DATA
Unless otherwise noted, the data presented in this Profile are from three national surveys of the United States civilian non-institutionalized population. The National Health Interview Survey (NHIS), conducted annually by the National Center for Health Statistics, is the principal source of information on the health of the U.S. population. The NHIS asks respondents whether a doctor has ever told them they have emphysema or if a doctor has told them during the previous year that they have chronic bronchitis. The 1998 Medical Expenditure Panel Survey (MEPS), cosponsored by the Agency for Healthcare Research and Quality and the National Center for Health Statistics, provides national estimates of health care use, expenditures, sources of payment, and insurance coverage. The MEPS asks respondents to report any current medical conditions. The 1998 Health and Retirement Study (HRS) provides information about the population age 51 and older. The HRS is sponsored by the National Institute on Aging and conducted by the Institute for Social Research at the University of Michigan. The HRS asks respondents if a doctor has ever told them they have chronic lung disease such as chronic bronchitis or emphysema.
ABOUT THE PROFILES
This is the second set of Data Profiles in the series, Challenges for the 21st Century: Chronic and Disabling Conditions. The series is supported by a grant from the Robert Wood Johnson Founda-tion. This Profile was written by Susan Rogers with assistance from Lee Shirey. Previous Profiles in this series include:
1. Screening for Chronic Conditions: Underused services
2. Childhood Obesity: A lifelong threat to health
3. Visual Impairments: A growing concern as the population ages
4. Cancer: A national concern
5. Prescription Drugs: A vital component of health care
The Center on an Aging Society is a Washington-based non-partisan policy group located at Georgetown University’s Insti-tute for Health Care Research and Policy. The Center studies the impact of demographic changes on public and private institutions and on the economic and health security of families and people of all ages.