



Screening for Chronic Conditions
Visit profiles to view data profiles on chronic and disabling conditions and on young retirees and older workers.
Underused services
Screening to identify people who have chronic conditions or are at risk of developing them can help prevent disease or lessen the severity of illness. Early detection and intervention can save money and lives.(1) The use of screening tests has increased in the U.S. in recent years, but not everyone who needs screening services receives them.(2) Although rates differ by condition, certain groups generally are less likely to be screened: people who do not have health insurance or a usual source of health care, those with lower incomes and those living in rural areas. Chronic conditions or risk factors for chronic con-ditions can be detected during routine physical exams. Discussions during physical exams about risk-related behaviors are an important screening tool. Clinical tests have been developed to screen for specific conditions, such as cancer, or for risk factors such as high cholesterol. Screening services also may be available in the workplace and other non-medical settings.
People with health insurance are more likely to have routine physical exams
One factor that is closely associated with whether adults receive routine medical care is whether they have health insurance. Adults with public and private health insurance, for example, are much more likely than adults who do not have insurance to get a checkup. Routine care also is more common among adults who have a usual source of care. More than half of adults who have a regular health care provider — 52 percent — report that they had a checkup within the last year, compared to only 28 percent of adults who do not have a usual source of care. People who have a usual source of care tend to have higher incomes and higher rates of insurance than others.
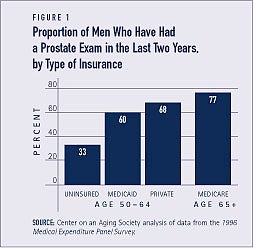
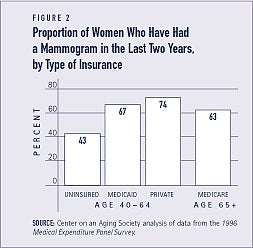
Health insurance is associated with screening for cancer
Men and women with private health insurance are most likely to be screened for prostate and breast cancer. Those who do not have insurance are least likely to be screened. Privately insured men age 50 to 64, for example, are more than twice as likely as uninsured men the same age to be screened for prostate cancer (see Figure 1).
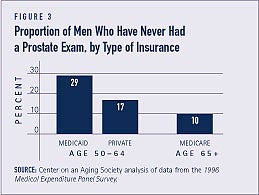
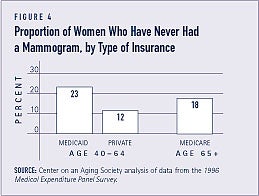
Insurance coverage does not guarantee screening
Adults who have health insurance do not always receive screening services. For example, some 2.3 million insured men age 50 to 64 have never been screened for prostate cancer. Similarly, 4.1 million insured women age 40 to 64 have never had a mammogram. One reason for low screening rates is that insurance may not cover certain procedures. Medicare coverage for preventive services is relatively recent, for example, with many of the benefits added by the Balanced Budget Act of 1997.(3) Also, people may not be screened for chronic conditions because they fear the results. Uncertainty about the effectiveness of treatment or the availability or affordability of follow-up services may also keep people from using screening services.
Screening for cancer is more common among certain populations
Regardless of the type of cancer, screening rates are consistently higher for people with higher incomes. Whites are more likely than blacks to be screened for cancer and urban residents have higher rates than rural residents. Marital status also appears to be associated with screening rates for cancer. People who are married are more likely to be screened (see Figure 5).
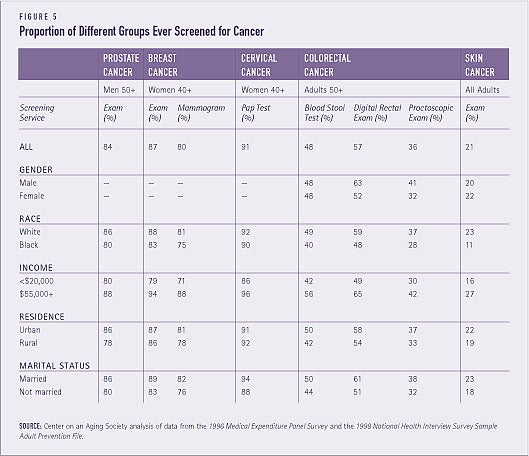
Screening rates differ by type of cancer
The proportion of the population that is screened for different types of cancer varies considerably. Some 91 percent of women age 40 and older, for example, have had a pap smear to check for cervical cancer. The proportions of men who have had prostate exams and women who have had breast exams are fairly high — over 80 percent. Rates are much lower for the screening tests related to colorectal cancer. And although skin cancer is the most common form of cancer in the U.S., the lowest screening rates are for skin cancer. Only 21 percent of adults report that they have ever been checked for skin cancer (see Figure 5).(4)
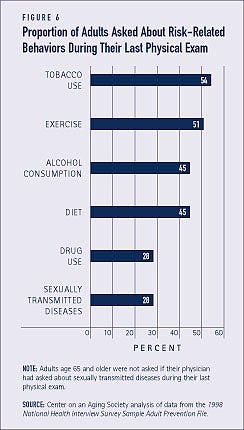
Only about half of adults are asked about risk-related behaviors
Questions about risk-related behaviors are asked during the course of some routine physical exams, but the practice is not universal. Only about half of adults report that they were asked about any risk-related behaviors during their last checkup. Physicians who do discuss health-related behaviors are more likely to ask about tobacco use, exercise, diet, and alcohol consumption. Discussions about sexually transmitted diseases and drug use are less common (See Figure 6).
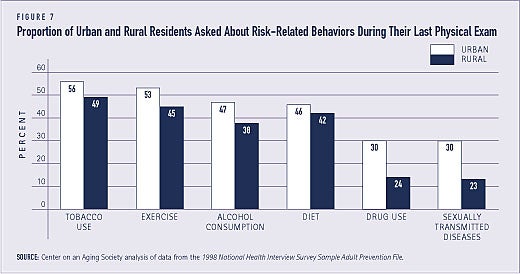
Some groups are more likely to be asked about risk-related behaviors
Physicians tend to ask certain groups about risk-related behaviors more frequently than others. Men are generally more likely than women, for example, to be asked about exercise, alcohol consumption and tobacco use. Larger proportions of black patients are asked about their diet, alcohol consumption, drug use, and sexually transmitted diseases than white patients. Routinely, patients in urban areas are more likely than patients in rural areas to be asked about all risk-related behaviors (see Figure 7).
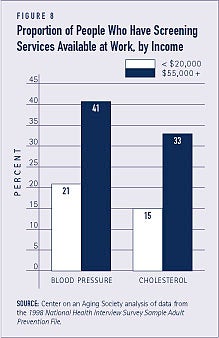
Screening services are more available for high-income workers
Screening for certain conditions and risk factors, such as high blood pressure and cholesterol, is available in some workplace settings. People with higher incomes are about twice as likely as those with lower incomes to have screening services for these risk factors available at work. Some 41 percent of higher-income workers have screening services for high blood pressure available at work compared to just 21 percent of lower-income workers (see Figure 8). Yet, the low-income population is more likely to have high blood pressure. There are not large differences, by income, in the proportion of the population with high cholesterol.
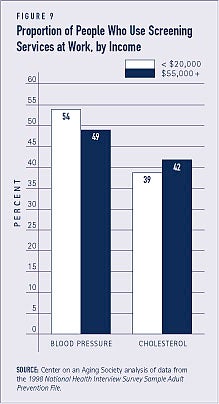
Workers of all incomes use screening services when they are available at work
About half of workers who have screening services for blood pressure available at work have used the services. This is true regardless of income. Close to two in five people who work in settings where cholesterol screening is available use it. The difference in the use of services by the lower and higher income groups is not great (see Figure 9). When screening services are available at work, use is higher among men than women and is higher among rural than urban residents.
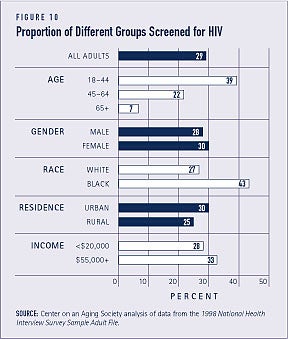
Almost one-third of adults have been tested for the AIDS virus
Almost 30 percent of adults report that they have had their blood tested for HIV, the AIDS virus. Younger adults are more likely than older adults to have been tested. Testing for AIDS is more common among the black population than the white population — 43 percent and 27 percent respectively. And, a larger proportion of urban than rural residents have been tested.
1. Centers for Disease Control and Prevention. (2000). Unrealized Prevention Opportunities, Reducing the Health and Economic Burden of Chronic Disease.
2. Coffield, A., M. Maciosek, J.M. McGinnis, J Harris, M.B. Caldwell, S. Teutsch, D. Atkins, J. Richland, A. Haddix. (2001). Priorities Among Recommended Clinical Preventive Services, American Journal of Preventive Medicine, 21(1).
3. Scala, Marisa. (2001). Medicare Preventive Services, Center for Medicare Education, Issue Brief, Volume 2, Number 5.
4. Centers for Disease Control and Prevention. (2001). Skin Cancer: Preventing America’s Most Common Cancer, 2001. Available at http://www.cdc.gov/cancer.
ABOUT THE DATA
Unless otherwise noted, the data presented in this Profile are from two national surveys of the United States civilian non-institutionalized population. The National Health Interview Survey (NHIS), which is conducted annually by the National Center for Health Statistics, is the principal source of information on the health of the U.S. population. The 1998 NHIS consists of several data files including the Sample Adult and the Sample Adult Prevention files. The 1996 Medical Expenditure Panel Survey (MEPS) is cosponsored by the Agency for Healthcare Research and Quality and the National Center for Health Statistics. It provides national estimates of health care use, expenditures, sources of payment, and insurance coverage.
ABOUT THE PROFILES
This is the second set of Data Profiles in the series, Challenges for the 21st Century: Chronic and Disabling Conditions. The series is supported by a grant from the Robert Wood Johnson Foundation. This Profile was written by Laura Summer with assistance from Lee Shirey and Craig Salman. It is the first in the new series.
The Center on an Aging Society is a Washington-based nonpartisan policy group located at Georgetown University’s Institute for Health Care Research and Policy. The Center studies the impact of demographic changes on public and private institutions and on the economic and health security of families and people of all ages.