



Substance Abuse: Facing the Costs
Visit profiles to view data profiles and issue briefs from the series Challenges for the 21st Century: Chronic and Disabling Conditions as well as data profiles on young retirees and older workers.
Substance abuse is a preventable and treatable condition that imposes tremendous financial and social costs. Societal costs of tobacco, alcohol, and illicit drug use are nearly 6 percent of the nation’s income — over $532 billion a year.(1) Educating people about the risks of using addictive substances, financing treatment for those who are addicted, and making it harder to obtain addictive substances are among the ways in which public policies have been used to reduce these costs. Success, however, has been limited. Over most of the past decade adolescent use of addictive substances increased, even while the trends among adults were decreasing. Policy makers have found the greatest success in discouraging adolescents from using addictive substances in multi-faceted community-wide efforts.
The Costs of Substance Abuse
Substance use is big business. Revenues from the sale of cigarettes, alcohol, and illicit drugs exceeded $128.3 billion or 2.5 percent of GDP in 1998.(2) About 11 percent of revenues from the sale of cigarettes and alcohol are used for advertising which amounts to over $10 billion a year, or $28 million a day.(3)
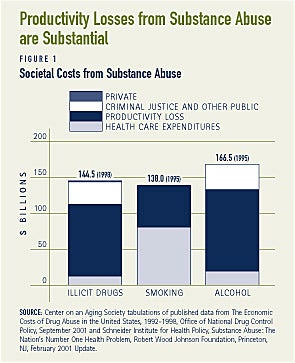
The societal costs of substance abuse in disease, premature death, lost productivity, theft and violence, including unwanted and unplanned sex, as well as the cost of interdiction, law enforcement, prosecution, incarceration, and probation are, however, greater than the value of the sales of these addictive substances (see Figure 1.) Everyone pays for these costs. Consumers pay in the form of higher prices for goods and services. Employers and employees pay higher health insurance premiums. Taxpayers pay higher taxes for the public expenditures of health care, law enforcement, the judicial system, incarceration as well as prevention and treatment programs. The price is also reflected in the need for foster care and homeless shelters. Substance abuse also hinders economic growth and diverts resources away from future investments.
Most of the adverse health consequences of substance abuse result in diseases and premature deaths. About 28 percent of all deaths annually can be traced to the use of tobacco, alcohol, or illicit drugs. Of these deaths, tobacco is directly responsible for the largest share. Alcohol and illicit drugs also lead to death directly, but are more likely to contribute to a fatal accident or homicide. Death from substance abuse is more likely to occur as an adult from substance use that began in adolescence.
What is Substance Abuse?
Substance abuse is the problematic use of alcohol, tobacco, illicit drugs or the deliberate misuse of legal drugs. It is a chronic disease of the brain. Substance abuse is an addiction, which is not only preventable but also treatable. Addiction is characterized by compulsive drug seeking that results from the brain’s prolonged exposure to specific chemicals. The process of becoming addicted is complex and is related to a multitude of confounding factors, including the particular substance as well as characteristics of the abuser. Personality, culture, family and peer influences, as well as existing psychiatric disorders and genetics can have a predisposing influence on who is more likely to become addicted.
Public Policies Aimed at Combating Substance Abuse
Public policies to combat substance abuse generally fall within one of the following categories:
• Discouraging people, particularly adolescents, from using addictive substances.
• Making it harder to obtain addictive substances.
• Helping those who are addicted quit.
Discouraging adolescents from starting
The younger people are when they first try a substance, the greater the likelihood that they will abuse that substance at some point. The longer they continue using a substance, the more likely they will have an accident or develop a fatal disease. More than 62 percent of illicit drug dependent adults started using an illicit drug at age 14 or younger.(4) Over 40 percent of those who began drinking before age 15 become dependent on alcohol, compared to 10 percent of those who begin drinking at age 21.(5) Over 90 percent of lifetime smokers first began smoking before age 18.(6)
Discouraging adolescents from starting requires social marketing, teaching about the risks and use patterns, showing them how to constructively say no, and applying moral suasion. Multi-pronged community-based programs that include the school, parents, and targeted counter-advertising, have been shown to be effective at getting adolescents to substantially delay or avoid trying addictive substances.7 Critical components of these efforts include one-on-one screening and counseling, school-based programs, and advertising to portray the dangers or to mitigate the pressures of trying these substances. Effective educational programs tend to focus on letting kids know that not everyone uses such substances and providing usable skills to resist temptation. Role-playing, videos, and workbooks help kids say “no” in a positive way. Information helps them to recognize that the vast majority of their peers are not using these substances. Adolescents are more likely to want to use these substances if they perceive that many of their peers are. Children whose parents are actively involved with their lives are much less likely to experiment with addictive substances.
It Takes a Community…
Evidence is emerging that makes it clear that a comprehensive school-based program works best but that such programs work even better when they are a part of a broader community-based effort directed at all ages. Key elements include multiple in-school sessions, sustained over the middle-school years, that focus on factual information and basic life-skills applied to resisting temptation; screening to identify particularly high risk adolescents with follow-up counseling; state-wide but community-reinforced efforts that provide counter-advertising, education to the general public and reminders with informational resources to health care providers; and vigilant enforcement of laws governing the sale of tobacco and alcohol to underage customers.
Such efforts require resources and hence schools unable to finance fundamental education cannot be expected to take on extensive substance abuse curricula. California, Massachusetts, Arizona, Florida, and Oregon are examples of states that have made reducing tobacco use a statewide priority.
Studies of their statewide tobacco campaigns overall as well as separate studies of their school-based efforts have shown dramatic results. In Oregon, for example, per capita cigarette consumption decreased 11.3 percent and prevalence rates among adults decreased 6.4 percent.(8) Cigarette use among 8th graders was down overall, but down substantially more in schools that had tobacco-free policies, family involvement, community involvement, tobacco prevention curriculum and instruction, teacher/staff training, and student tobacco use cessation support.(9) The Substance Abuse and Mental Health Services Administration of the Department of Health and Human Services found that school-based substance abuse programs in communities that were making use of the community partnership federal grants were also more effective at reducing alcohol and illicit drug use than in communities that did not have such efforts.(10)
Making it harder to obtain addictive substances
Social marketing, the skills and confidence to say no, and moral suasion are not likely to be sufficient to keep adolescents from using addictive substances. Other limits to addictive substances may also be necessary.
They include:
• Making it illegal to produce or distribute the product.
• Making it illegal to purchase the product, either for everyone or for those under a certain age (and also limiting the sites at which legal purchases are permitted).
• Raising the price of the product, usually by imposing an excise tax.
The extent to which these different approaches are applied and enforced varies with the substance and across jurisdictions. Illicit substances call for the most law enforcement activity. As a consequence, 63 percent of all prisoners are in prison for producing, distributing, or purchasing an illicit substance.(11)
Efforts to limit access to legal substances for those under specific ages have had limited success. It requires vigilance on the part of authorities to ensure that store operators follow the law. In a 1995 survey of youth, the majority of teens were able to purchase cigarettes without being asked for proof of their age.(12)
Federal, state and local excise taxes have been used to not only raise revenue but to discourage the purchase of tobacco and alcohol. Neither federal nor state excise taxes automatically increase with the cost of living and in fact are considerably less in real terms than when they were first imposed. Total excise taxes on cigarettes, as a proportion of the retail price, are less than 12 percent in the United States, whereas in Argentina, France, and Spain, for example, the tax is more than 50 percent of the retail price.(13)
Each of these activities–raising the excise tax, raising the legal age, channeling purchases to particular sites such as liquor stores, or eliminating vending machines–have all had measurable effects on consumption of cigarettes and alcohol. In the extreme, alcohol consumption was dramatically lower during prohibition. More recently, alcohol consumption declined when the legal drinking age was raised from 18 to 21. Adolescent smoking is now at a 10-year low, in part due to the dramatic increase in the price of cigarettes.(14) However, teenagers are still able to obtain substances that are illegal for them to purchase.
Treatment for addiction
Prevention and limits on access have not stopped some people from becoming addicted. Treatment for addiction can work and is less expensive than either incarceration or lost productivity and property. However, in order to work, treatment must be easily available and encouraged. Unfortunately the treatment process takes time and for youth, it is most effective when family members participate.
Evaluations of smoking cessation programs have shown that FDA-approved medications used in combination with clinically provided social support and skills-training or problem solving programs, reinforced by employer no-smoking policies result in the highest long-term smoking cessation rates.(15) Alcohol and drug dependency programs have also been found to be effective. Treatment of illicit drug use has been shown to reduce drug use by 40 to 60 percent and significantly decreases criminal activity.(16)
Programs to help those dependent on alcohol, drugs, or cigarettes are not
widely available. In fact, demand for such programs far exceeds their availability. In large part this is because of the way treatment programs have been financed. While most health care is either insured or covered by public
health care programs, dependency treatment programs are often not included. About 70 percent of funding for alcohol and drug treatment programs is publicly funded, however, less than one-quarter of this public funding is through either Medicaid or Medicare. Private insurance plans finance 14 percent, clients finance 10 percent, and charities fund the remaining 5 percent.(17)
Most employer-provided health insurance plans do not cover treatment, and many that do have limited coverage. Medicare too, while more extensive than most private insurance plans, leaves the scope of coverage, on a case-by-case basis, to each of Medicare’s fiscal intermediaries. Medicaid coverage also varies by state. Smoking cessation programs are even less likely to be covered. Smoking cessation is not covered by Medicare, or by half of the state Medicaid programs.(18)
It is not uncommon for people with a substance abuse problem to also have a mental health disorder. Some 53 percent of drug abusers and 36 percent of alcohol abusers have at least one mental health problem.(19) For most of these persons (80 percent) the mental disorder preceded the substance abuse. For this reason, coverage of mental health is just as important as coverage for the treatment of addiction. Insurance plans and public programs with limited coverage of substance abuse treatment are likely to also have severe limits on mental health coverage.
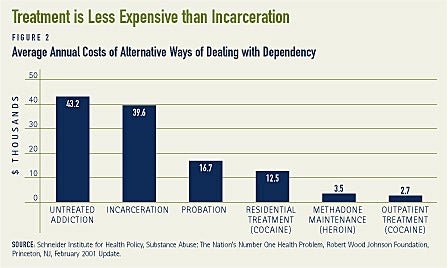
Those who seek treatment need as much support as possible, yet access to treatment is limited. People can spend months waiting to gain access to a program and many smaller communities have no programs. Lack of coverage and lack of resources limit the duration of treatment and the number of times one can seek treatment. It is not uncommon for people to require multiple efforts of treatment before they are fully treated. Ironically, treatment for alcohol and drug abuse is far less expensive than the societal costs. An Institute of Medicine study, for example, estimated that the cost per person per year of outpatient treatment for cocaine or heroin was about $3,100. Residential treatment for cocaine was about $12,500. Untreated addictions, however, were estimated to cost $43,200 per year per person, mostly due to the cost of incarceration ($39,600 per year per person) (see Figure 2).(20)
Combating Substance Abuse: Three Steps Forward and One Step Back
Some of the efforts to reduce substance abuse have been successful. However, substantial numbers of people are still abusing addictive substances. Moreover, the trends among adolescents have not always been consistent with the trends among adults. In fact for most of the past 15 years, adolescent use was increasing even when use among adults was declining. Only in the past year or two have trends for adolescents and adults declined for most addictive substances.
Variation in the trends over time reflects attitudes about substances as well as the specific efforts taken to discourage use. A review of these trends suggests just how important effective prevention and treatment can be. For example, in 1964 the Surgeon General issued a report that declared cigarette smoking as harmful to one’s health. The Surgeon General’s warning was then required to be placed on each pack of cigarettes. Undertaking the research to support the warning and requiring that the warning be advertised was a relatively inexpensive form of prevention that had a significant impact on reversing a more than 60-year trend in the per capita consumption of cigarettes. The introduction of the nicotine patch in 1991 significantly helped smokers reduce their consumption and cease their dependence.
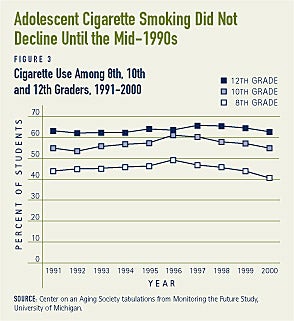
CIGARETTE USE. Efforts directed at limiting underage access to cigarettes have not been as successful. Advertising directed at encouraging underage smoking was more effective than the counter-advertising and the restrictions imposed on the sale of cigarettes. Only in the last few years, when cigarette advertising was significantly curtailed, has the trend in underage smoking begun to follow the smoking trends among adults (see Figure 3). This is in part a response to the ban on direct advertising, but it is also in conjunction with increased and concerted school and community-based efforts to discourage adolescents from smoking as well as higher prices for cigarettes.
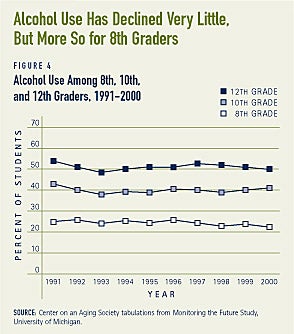
ALCOHOL USE. Overall, per capita alcohol consumption has been declining since 1980. Most of the decline has been in the use of distilled spirits. It is probably not a coincidence that during much of this time the distilled liquor distributors voluntarily stopped advertising on radio and television. In 1997, distilled liquor advertising returned to television and radio, but pressure from Congress and special interest groups, have recently led television networks to reconsider allowing advertising for distilled liquor. In the meantime, community-based advocacy and education groups, like Mothers Against Drinking and Driving (MADD), have become increasingly more effective at influencing school-based efforts to not only educate students but to also sponsor alcohol free alternatives on the weekends. The social marketing impact of these efforts has raised consciousness concerning drinking and driving and contributed to the decline in alcohol use itself. Alcohol use among 8th graders has consistently declined through out the 1990s and it declined somewhat for 12th graders, but not for 10th graders (see Figure 4).
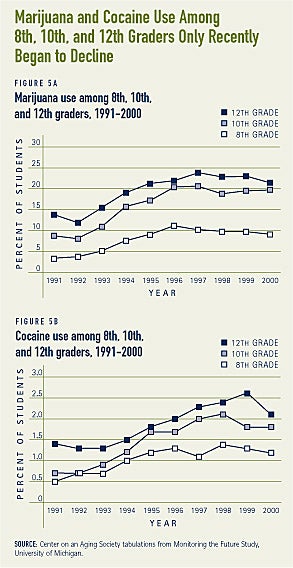
ILLICIT DRUG USE. While the proportion of the whole population using marijuana and cocaine has declined, the percent of 8th, 10th, and 12th graders using marijuana or cocaine increased during most of the 1990s (see Figure 5). Only in the past few years, when more community-based efforts began, has there been an apparent reversal of these trends among adolescents. Heroin use among all ages has been relatively constant over the past decade. However, the use of MDMA (ecstasy) and methametaphines has been increasing among adolescents and adults.
Lessons Learned
With the clear exception of methametaphines and MDMA, the use of tobacco, alcohol, and other illicit drug use among adolescents and adults has declined over the past few years. While a change in a trend can mark success, it is a bit too soon to declare victory. Per capita consumption of tobacco is still greater than it was in the early 1940s and per capita consumption of alcohol is about what it was in 1965. Cocaine and marijuana use, although down among adults, is similar to use in the late 1980s. More disconcerting is that despite well-publicized deaths, binge drinking among college students does not seem to have changed at all. More than 40 percent of college students report that they have engaged in binge drinking in the past 2 weeks.(21)
The trend data in conjunction with a review of efforts to combat substance abuse make it clear just how important it is to discourage adolescents from trying addictive substances. Efforts that focus on reducing demand tend to be more effective than efforts to limit access to supply. This does not mean that efforts to limit supply have been ineffective, merely that the next dollar expended in prevention and treatment may be worth more than the next dollar expended on law enforcement and interdiction.
There is little question that without concerted efforts to disrupt production and distribution the supply of illicit drugs would be greater than it otherwise is. However, there is sufficient supply of illicit drugs to not only meet existing demand but to do so at a lower price than in the past.
Despite the interdiction and law enforcement efforts, the average “retail” price of cocaine, heroin, marijuana, and methamphetamine is lower, in both nominal and real terms, today than 10 years ago. For legal substances, excise taxes on cigarettes and alcohol and more vigilant enforcement of existing laws prohibiting the sale of these substances to minors has been shown to help hinder access by youths.
A Note of Concern about Baby-Boomers
The Substance Abuse and Mental Health Services Administration has identified substance abuse among older people as an “invisible epidemic.” Substance abuse, particularly of alcohol and prescription drugs, is one of the “fastest growing health problems facing the country.”(22) Between 1995 and 1999, admissions at publicly financed treatment centers for illicit drugs increased by 25 percent for men and 43 percent for women age 55 and older.(23)
The public health concern stems from a number of different perspectives. Despite the rapid growth in the population age 60 and older, there has been relatively little effort to identify, diagnose, or treat this population. Insufficient data and hence awareness among health care providers, aided by peer disproval and individual shame, has kept this issue invisible. Of greater concern is the fact that drug and alcohol abuse take a greater health care toll on older people due to biomedical changes and a greater likelihood of drug interactions with prescription drugs.
Those now age 60 and older experienced adolescence and young adulthood during the decades in which both alcohol use and illicit drug use were among the lowest in history. Yet an estimated 17 percent of the population age 60 and older reports abusing alcohol, prescriptions or illicit substances.(24) Because of the strong link between substance abuse and substance use at younger ages as well as the connection between substance abuse and societal attitudes about substance use, public health officials are concerned. More than one-half of baby boomers were adolescents and young adults during the 1960s and 1970s when cigarette and alcohol use were at historically high rates of per capita use. Illicit drug use was rising substantially during the 1960s and reached a historic peak in the 1970s. Moreover, societal attitudes about substance use were among the most permissive during these decades. Hence public health officials are concerned that the proportion of older people abusing alcohol, prescriptions, or illicit drugs will increase. Even if the proportion of older people abusing substances remains the same, the shear growth in the number of people age 65 and older ensures that there will be more older people with a substance abuse problem. Only if trends of substance use among future cohorts of adolescents decline, can we be more confident that future trends in substance abuse among older people will also decline.
1. Estimates of the economic costs of alcohol abuse, smoking, and drug abuse were $166.5 billion, 138.0 billion, and 109.9 billion, respectively, in 1995. Schneider Institute for Health Policy, Substance Abuse: The Nation’s Number One Health Problem, Robert Wood Johnson Foundation, Princeton, NJ, February 2001 Update. The total, or 414.4 billion was over 6 percent of GDP in 1995. The estimate reported here is based on applying the 6 percent of GDP to the GDP of 2001.
2. Author’s calculations based on What America’s Users Spend on Illegal Drugs, December 2000, Office of National Drug Control Policy and Statistical Abstract of the United States, Government Printing Office, Table 734, 2001.
3. Tobacco Advertising and Promotion Fact Sheet, Surgeon General’s Report on Reducing Tobacco Use, 2002, and Community Anti-Drug Coalitions of America and the Center for Science in the Public Interest, Alcohol Advertising: Its Impact on Communities, and What Coalitions Can Do to Lessen That Impact, http://www.cspinet.org/booze/Alcohol_Advertising.pdf.
4. Office of National Drug Control Policy, July 2001.
5. Grant, B. F., and D.A. Dawson. “Age at onset of alcohol use and it s association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiological Survey.” Journal of Substance Abuse, 9 (January, 1998.): 103
6. National Household Surveys on Drug Abuse (1998), unpublished data. Also, U.S. Department of Health and Human Services, Preventing Tobacco Use Among Young People: A Report of the Surgeon General (1994).
7. Botvin, G.J. Griffin K. W. Diaz, T and M. Ifill-Willams. “Drug abuse prevention among minority adolescents: Posttest and one-year follow-up of a school-based preventive intervention,” Prevention Science, 2(1), 1-13, 2001.
8. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, Feb 26, 1999 48 (07); 140-143.
9. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, August 10, 2001 50(31); 683-6.
10. SAMHSA/CSAP’s National Evaluation of Community Partnerships, DHHS Publication No. (SMA) 00-3373, 2000.
11. Substance Abuse: The Nation’s Number One Health Problem.
13. World Health Organization, www5.who.int/tobacco/index.cfm
14. Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report, May 17, 2002, Vol. 51, No. 19.
15. U.S. Public Health Service Report, Treating Tobacco Use and Dependence: A Clinical Practice Guideline, Journal of the American Medical Association, 1999.
16. Office of National Drug Control Policy, The National Drug Control Strategy: 2001 Annual Report.
17. Substance Abuse: The Nation’s Number One Health Problem, 2001.
19. Blose, J.O. and H.D. Holder (1991) “Psychiatric Co-morbidity and Suicidality Among Intravenous Drug Users.” American Journal of Public Health 81:1571. Berman, M. O. (1990) “Severe Brain Dysfunction: Alcoholic Korsakoff’s Syndrome.” Alcohol Health Research World, 14(2): 120-129, as cited in “Alcoholism and Co-occurring Disorders,” Alcohol Alert, No. 14, PH302, October 1991.
20. Substance Abuse: The Nation’s Number One Health Problem.
21. Panel on Contexts and Consequences report to the Task Force on College Drinking, High Risk Drinking in College: What we Know and What We Need to Learn, National Institute on Alcohol Abuse and Alcoholism, Washington, DC, April 2002.
22. SAMHSA, U.S. Department of Health and Human Services, Substance Abuse Among Older Adults, Treatment Improvement Protocol Series 26, DHHS Publication No. (SMA) 98-3179, 1998.
23. Christian Science Monitor, Illicit Drug Use Grows Among the Elderly, March 27, 2002. Admissions for people age 50 and older for alcohol abuse at these public facilities, however, declined by 9 percent.
24. The National Household Survey on Drug Abuse, 1999.
ABOUT THE ISSUE BRIEFS
This is the first in a series of Issue Briefs on Challenges for the 21st Century: Chronic and Disabling Conditions. This series is supported by a grant from the Robert Wood Johnson Foundation. The Issue Briefs accompany the Center’s ongoing series of Data Profiles in the same series. Robert Friedland wrote this Issue Brief with assistance from Lee Shirey and Brendan Kiel.
The Center on an Aging Society is a non-partisan policy group located at Georgetown University’s Institute for Health Care Research and Policy. The Center studies the impact of demographic changes on public and private institutions and on the financial and health security of families and people of all ages.